
Why you clench your jaw.
Your jaw isn't broken. Your jaw is reporting.
Your night guard protects your enamel. It does nothing about why you clench.
You’ve been told you clench because you’re stressed. You probably are. But if stress were the whole story the night guard would have worked by now — and for most people it just quietly becomes permanent.
Here’s what changed my mind about this letter. I went looking for the evidence that your bite causes your clenching, and I found that the field’s own authorities had gone looking too, and come back with nothing. That sounds like it should have gutted the piece. It did the opposite. It cleared away a story I never needed and left a better one standing.
Originally sent to AER members as an email. The exact send date wasn’t recovered — the date shown reflects publication order, not a precise record.
Before you read anything — 30 seconds
One check, and it isn’t your teeth
Freeze. Don’t fix anything yet. Were your teeth touching just now? At rest they’re meant to be apart — lips closed, teeth not in contact. If they were touching, some part of you was already working.
Now the real question: what else was on? Before you relax the jaw, take inventory. Where was your breath — high in the chest, or low and quiet? Were your shoulders up near your ears? Had you stopped breathing altogether while you read that last paragraph?
Whatever you just found — the shallow breath, the lifted shoulders, the ribcage holding still — that’s the subject of this letter. The jaw was just the part loud enough to notice.
The short version
Your night guard protects your enamel. It does nothing about why you clench.
We’ve known that for a while, and not as a suspicion. When researchers gave bruxers a full-arch splint and actually watched what happened, the splint did not stop the bruxing. The wear marks came back — same place, same pattern, visit after visit.1
Sit with that, because it’s the whole letter in one finding. Cover the teeth and the behaviour goes right on happening, unchanged, in the same shape. Whatever is driving this is not in your mouth. It’s upstream. The mouth is just where it becomes visible.
Your jaw isn’t broken. Your jaw is reporting.
The story I’m not going to tell you
Let me kill something first, because you’ve probably been sold it — and because I used to lean on it myself.
Your bite is not causing your clench. In 2012, four of the field’s leading bruxism researchers — the same group that writes the international consensus statements — reviewed the literature specifically to test that idea. Forty-six papers. Their conclusion, word for word: “there is no evidence whatsoever for a causal relationship between bruxism and the bite.”3 Not thin evidence. None. Neither occlusal interference nor the anatomy of your jaw is implicated in why you brux.
And your bite doesn’t predict your posture either. A systematic review and meta-analysis asked whether head and neck posture track with malocclusion, and concluded the evidence is “not sound enough to prove the association.”12
So: no mechanical fault in the bite, and no population-level line from your bite to your posture. If that’s what you came for, I don’t have it — and neither does anyone else who has actually checked.
Good. Here’s what is there.
What replaced it is more interesting
Bruxism is centrally regulated. Not peripherally. That’s the literal title of the paper, and it has held for twenty-five years: morphological factors — the shape of your teeth, the bones of your face — “play only a small role, if any.” Attention moved to the brain, to arousal during sleep, and to the neurotransmitter systems that modulate jaw motor activity.2
Then the field went further, and this is the part I find genuinely clarifying. The international consensus on bruxism concluded that in otherwise healthy people it should not be considered a disorder at all — but rather “a behaviour that can be a risk (and/or protective) factor” for certain outcomes.4
A behaviour. Possibly a protective one.
That’s the field’s own language, not mine. And it says the thing AER says about nearly every other joint in the body: the thing you want to eliminate is very often the thing holding you together. You don’t get to just delete it. You have to make it unnecessary.
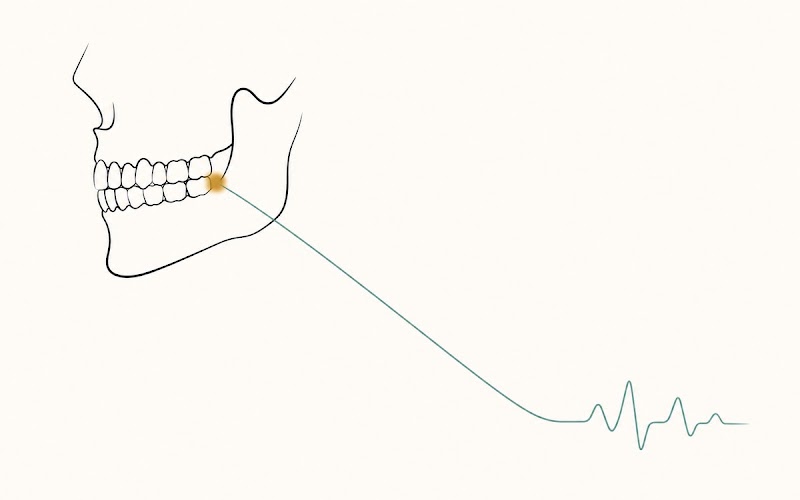
The timing is the proof
Here’s what actually convinced me, and it’s a matter of clock time.
Researchers wired bruxers up overnight and watched the sequence around each episode. What happens first isn’t the jaw.
About eight minutes before the jaw does anything, the balance of the autonomic nervous system starts shifting toward sympathetic — the accelerator side.6
About four seconds before the jaw does anything, the cortex lights up. In 79% of episodes.5
About one heartbeat before the jaw does anything, heart rate climbs.5
Then the jaw moves.
Brain. Heart. Then jaw. The jaw is the last link in the chain, not the first — and nothing can cause an event that already started eight minutes earlier. Whatever your bite is doing down there, it is not reaching backwards in time to accelerate your heart.
That’s what I mean when I say the jaw is reporting. It’s a readout of a nervous-system state that was already on the move before your teeth ever came together.
And it isn’t chewing
One more detail that gives the game away.
When you chew, your jaw-opening and jaw-closing muscles alternate. Open, close, open, close — like everything else your body does well.
During sleep bruxism they fire together.7 Openers and closers, co-contracting. That is not a chewing pattern. That’s the signature of a system splinting itself — the same thing a body does around a joint it doesn’t trust.
And the same review notes this rhythmic jaw activity turns up in roughly 60% of normal sleepers who don’t grind at all.7 The machinery is standard-issue human. In bruxers, the volume is just turned up.
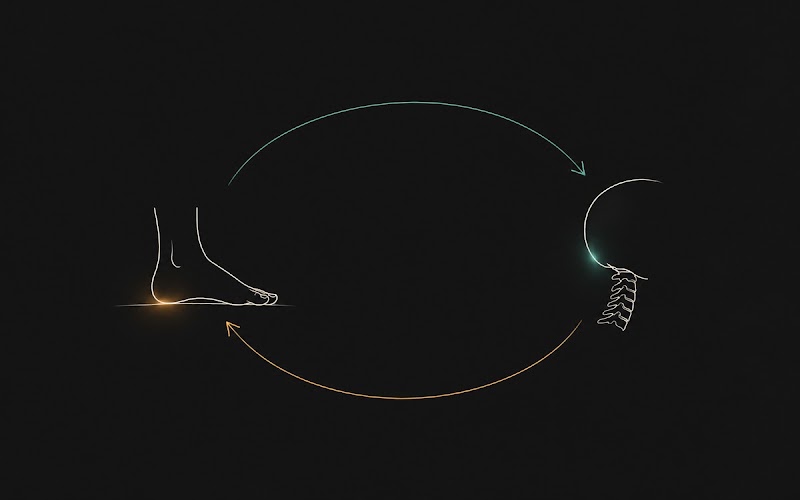
How the system talks to itself
So if the jaw is downstream of a whole-body state — is it actually wired to the rest of you? Yes. And this is the part that’s genuinely well-measured.
Clench, and your neck goes with it. Ask someone to clench hard and neck muscle activity jumps to between 7.6 and 33 times resting level.8 Not a nudge. The jaw does not brace alone; it recruits the neck, every time.
Clench, and your weight moves. Put people on a pressure platform and have them clench on one side, and their body weight shifts away from the side they’re clenching on — left in 65% of people clenching right, right in 70% clenching left. Side to side only; front to back, nothing.9
And your teeth are sensors, not just tools. Every tooth hangs in a ligament packed with mechanoreceptors that encode how hard you’re biting and in which direction, and those signals feed straight into the fine motor control of your jaw. Pull the tooth and you don’t just lose a grinder — you lose the sensor, and the motor control degrades with it.10
Here’s the wrinkle worth sitting with. Those receptors are most sensitive at very low forces — under about 1 newton at the front teeth.10 They’re built for delicate contact: the instant food first touches. A hard clench is nowhere near that range. So a jaw that’s clamping down is not a jaw that’s getting good information — it’s operating well past the range where its own sensors are precise.†
Your bite is not a closed system that stops at your lips. It’s wired into how you stand, how you hold your neck, and how you feel the ground.
The warning label
I’ve just told you a clean story. Here’s where it’s thinner than it sounds, because you deserve the same footnotes I read.
Every one of those couplings is acute, not chronic. The neck-EMG study is 10 university students doing a hard voluntary clench in a lab.8 The weight-distribution study is 20 healthy adults with instability created on the spot by a 1 mm shim.9 They show that jaw, neck and stance are motorically wired together in the moment. They do not show that your habitual clench is reshaping your posture over years, and I’m not going to let them quietly imply it.
The step from “the jaw is an output of a system state” to “so change the state and the jaw lets go” is mine, and it’s PRI’s.† That’s a clinical inference, not a finding. It’s what I see in the room, repeatedly. It has not been tested in a trial — and the mechanical version of this idea has already been tested, and failed. File it accordingly.
Stress is real, but softer than its reputation. Stressed people show roughly twice the odds of bruxing (OR 2.07). But that pooled only three observational studies, and the authors graded their own certainty as low.13 It’s association, not causation, and it doesn’t rule out the arrow pointing the other way — or both being downstream of something else.
And don’t let me blur sleep and daytime. The consensus literature treats sleep bruxism and awake bruxism as distinct behaviours.4 The eight-minute autonomic run-up6 and the four-second cortical run-up5 were measured during sleep. They’re the cleanest evidence I know that the jaw is an output rather than an origin — but daytime clenching is its own animal, and I shouldn’t silently import one to explain the other. Neither should anyone else. Including me.
What this means
Telling someone who clenches to relax their jaw is like telling someone who limps to stop limping. The clench is there for a reason, and the reason isn’t in the tooth.
What I see on the training floor, again and again: when the state underneath gets addressed — the breath dropped out of the chest, the ribcage allowed to come down, the neck given something to do besides brace — the jaw lets go on its own. Not because I trained the jaw. Because I took away its job.†
That’s an observation from my own practice, not a trial. But it’s why I go looking below the mouth. And it’s why the first thing we change is how you breathe.
Two things you can try today
1. Work the state, not the jaw. The clench is downstream of arousal.2,5,6 So go upstream. Long, slow, complete exhales — longer out than in — until the exhale finishes on its own instead of getting cut short. Four or five of them. Then check the jaw.
You’re not stretching anything. You’re changing the input the jaw is responding to.†
2. Give the heel back to your gait. Plenty of people who clench land midfoot or forefoot — the heel skims the ground and the body’s already moving on. Slow your walk down and let each heel land fully before you roll through it.
Straight with you about what this is and isn’t. I am not claiming this trips a jaw reflex. The paper everyone cites for that used hopping and running, and concluded there is no reflex control of the jaw during ordinary walking — at a walk, the movements are too small and too slow to reach reflex threshold, and the jaw is simply held by the soft tissue around it.11 Anyone telling you a gentle heel-first stroll “activates your jaw reflex” is citing a paper that says the opposite.
What this drill actually is: a way to feel whether your heels are participating in your stance at all.† Most people are startled by the answer. Five minutes. Just notice.
Neither of these is a treatment. They’re both questions you’re asking your body, and the answers are the useful part.
Is this you
If the night guard quietly became permanent instead of temporary — now you know why it was never going to be temporary.
If your neck tension, your headaches and your jaw all seem to travel together — they do, and there’s a measured reason for it.
If you’ve had the nagging sense that the jaw is a symptom and not the source: you’re right. The evidence agrees with you. The source is a nervous system that hasn’t been given a reason to stand down — and nobody’s found it, because everybody’s been staring at your teeth.
The fine print
-
Holmgren K, Sheikholeslam A, Riise C. Effect of a full-arch maxillary occlusal splint on parafunctional activity during sleep in patients with nocturnal bruxism and signs and symptoms of craniomandibular disorders. J Prosthet Dent. 1993;69(3):293–297. PMID 8445561. The authors report plainly that the splint does not stop nocturnal bruxism; wear facets recurred in the same location with the same pattern, and were caused mainly by grinding. Limitation: a small clinical sample of patients already diagnosed with bruxism and craniomandibular disorders, using 1993-era methods. It establishes that the splint doesn’t stop the behaviour. On its own it does not establish where the behaviour comes from — that’s what notes 2–7 are for.
-
Lobbezoo F, Naeije M. Bruxism is mainly regulated centrally, not peripherally. J Oral Rehabil. 2001;28(12):1085–1091. PMID 11874505. Morphological factors — occlusal discrepancies and the anatomy of the orofacial bony structures — “play only a small role, if any”; the aetiology is centrally mediated, involving sleep arousal and central neurotransmitter systems (notably dopaminergic). Limitation: a narrative review, not a meta-analysis. Its central claim has nonetheless held for two decades and is reflected in the current consensus literature.
-
Lobbezoo F, Ahlberg J, Manfredini D, Winocur E. Are bruxism and the bite causally related? J Oral Rehabil. 2012;39(7):489–501. PMID 22489928. Forty-six papers reviewed. Conclusion, verbatim: “based on this review, it should be concluded that to date, there is no evidence whatsoever for a causal relationship between bruxism and the bite.” Neither occlusal interferences nor orofacial skeletal anatomy are implicated in aetiology; the authors note growing awareness of psychosocial and behavioural factors instead. Limitation: a critical review rather than a meta-analysis. But the negative finding is consistent, it comes from the field’s own authorities, and it has stood. I am citing it against my own tradition’s mechanical explanation. I’d rather you have it than not.
-
Lobbezoo F, Ahlberg J, Raphael KG, Wetselaar P, et al. International consensus on the assessment of bruxism: report of a work in progress. J Oral Rehabil. 2018;45(11):837–844. PMID 29926505. Bruxism is defined as masticatory muscle activity characterised by clenching or grinding and/or by bracing or thrusting of the mandible, specified as either sleep or awake bruxism — treated as distinct behaviours. The consensus concluded that in otherwise healthy individuals bruxism “should not be considered as a disorder, but rather as a behaviour that can be a risk (and/or protective) factor” for certain clinical consequences. Definitions were further revised in Verhoeff MC, Lobbezoo F, Ahlberg J, Bender S, et al. Updating the bruxism definitions: report of an international consensus meeting. J Oral Rehabil. 2025;52(9):1335–1342. PMID 40312776 — which removed the “in otherwise healthy individuals” addendum from the specific definitions of sleep and awake bruxism. Limitation: this is expert consensus — a statement of how a field agrees to define and grade a behaviour, not an experimental result. I’m using it for exactly what it is: the field’s own framing, in the field’s own words.
-
Kato T, Rompré P, Montplaisir JY, Sessle BJ, Lavigne GJ. Sleep bruxism: an oromotor activity secondary to micro-arousal. J Dent Res. 2001;80(10):1940–1944. PMID 11706956. Cortical EEG activity rose 4 seconds before the onset of jaw muscle activity in 79% of episodes, and heart rate accelerated one cardiac cycle before onset: “a clear sequence of cortical to autonomic-cardiac activation precedes jaw motor activity.” Limitation: 10 sleep-bruxism patients matched with 10 controls — a small sample. It establishes the order of events, which is the load-bearing point here — not the size of an effect, and not a cause.
-
Huynh N, Kato T, Rompré PH, Okura K, et al. Sleep bruxism is associated to micro-arousals and an increase in cardiac sympathetic activity. J Sleep Res. 2006;15(3):339–346. PMID 16911037. A shift in sympatho-vagal balance toward increased sympathetic activity began roughly 8 minutes before the onset of a bruxism episode (P ≤ 0.03); 75.8% of episodes occurred in clusters. Limitation: 60 subjects in three groups of 20, polysomnography across two nights. This is an association in time — an autonomic shift reliably precedes the jaw event. It is strong evidence about sequence*. It is not proof that the autonomic shift* causes the clench, and it was measured during sleep only.
-
Lavigne GJ, Kato T, Kolta A, Sessle BJ. Neurobiological mechanisms involved in sleep bruxism. Crit Rev Oral Biol Med. 2003;14(1):30–46. PMID 12764018. Sleep bruxism is mainly associated with rhythmic masticatory muscle activity (RMMA), observed in around 60% of normal sleepers without grinding sounds, and roughly three times more frequent and higher in amplitude in bruxers. RMMA is characterised by co-activation of jaw-opening and jaw-closing muscles, rather than the alternating pattern typical of chewing. Brainstem structures and neurochemical systems (serotonin, dopamine, GABA, noradrenaline) are implicated. Limitation: a review. The authors are explicit that key questions remain open — including why RMMA is so common in normal sleepers — and they float, as a hypothesis and not a finding, that RMMA may help lubricate the upper airway. I am not building anything on that hypothesis; I use only the co-activation and prevalence findings.
-
Ehrlich R, Garlick D, Ninio M. The effect of jaw clenching on the electromyographic activities of 2 neck and 2 trunk muscles. J Orofac Pain. 1999;13(2):115–120. PMID 10425983. Jaw clenching raised neck-muscle EMG (sternocleidomastoid, trapezius) to 7.6–33× resting activity; trunk muscles rose 1.4–3.3×. Limitation: 10 university students performing a strong voluntary clench in a lab, supine and sitting. It demonstrates that jaw and neck are motorically coupled during a hard clench. It does not measure habitual or nocturnal clenching, and the multiples should not be read as what your neck is doing all night.
-
Michalakis KX, Kamalakidis SN, Pissiotis AL, Hirayama H. The effect of clenching and occlusal instability on body weight distribution, assessed by a postural platform. Biomed Res Int. 2019;2019:7342541. PMID 31341904. Subjects shifted body weight opposite the clenching side — 65% shifted left when clenching right, 70% shifted right when clenching left. The effect was lateral only; the authors found no effect on anteroposterior weight distribution. Limitation: 20 healthy adults aged 27–40, all Angle Class I, with instability induced experimentally by a 1 mm disocclusion. An acute laboratory manipulation in a small sample — not a study of chronic clenchers — and the authors state that further clinical research is needed before definitive conclusions.
-
Trulsson M. Sensory-motor function of human periodontal mechanoreceptors. J Oral Rehabil. 2006;33(4):262–273. PMID 16629881. Periodontal receptors encode both the magnitude and the direction of tooth loads and feed the fine motor control of the jaw; they are most sensitive at very low force levels (below ~1 N for anterior teeth, ~4 N for posterior teeth); these sensory-motor functions are lost or impaired when teeth are extracted. Limitation: a review of microneurography studies in small samples, concerned with jaw motor control during mastication specifically. The low-force tuning is the paper’s own finding. The inference drawn in the text — that a hard clench therefore operates outside the range where those sensors are precise — is mine*, and is marked † as an interpretation, not a result the author reports.*
-
Miles TS, Flavel SC, Nordstrom MA. Control of human mandibular posture during locomotion. J Physiol. 2004;554(Pt 1):216–226. PMID 14678503. Heel-landing during hopping and running drove the mandible downward and evoked a masseter reflex at monosynaptic latency; toe-landing produced only small movements and no reflex. Limitation — and this one is load-bearing, so read it: during walking*, the authors found mandibular movements were “subthreshold for stretch reflexes in the jaw muscles,” with the mandible “supported by visco-elasticity of the soft tissues.” There is* no reflex jaw control during ordinary walking. Anyone citing this paper to claim a gentle heel-first walk “activates the jaw reflex” is contradicting the paper’s own conclusion. I’ve corrected that claim in the text above rather than repeat it.
-
Peng H, Liu W, Yang L, Zhong W, et al. Does head and cervical posture correlate to malocclusion? A systematic review and meta-analysis. PLoS One. 2022;17(10):e0276156. PMID 36282836. Conclusion, verbatim: “the current research evidence is not sound enough to prove the association of head and cervical posture with sagittal malocclusion.” Limitation: 6 cross-sectional studies, 505 participants, moderate methodological quality. Read it precisely — it says the association is not established*, which is not the same as* disproven*. It concerns posture and* malocclusion*, not posture and* bruxism*, and I’m not stretching it past what it measured.*
-
Chemelo VDS, Né YGS, Frazão DR, et al. Is there association between stress and bruxism? A systematic review and meta-analysis. Front Neurol. 2020;11:590779. PMID 33424744. Stressed individuals showed higher odds of bruxism (OR 2.07, 95% CI 1.51–2.83). Limitation, and it is the authors’ own: six studies reviewed but only three pooled in the meta-analysis, all observational — association, not causation, with reverse causation not excluded. The authors graded the certainty of the evidence as low. This is the citation behind the sentence everyone thinks is obvious, and it is softer than its reputation.
A note on earlier versions of this letter. Three corrections. I’m recording them here rather than quietly fixing them, because a letter whose whole premise is “check my footnotes” doesn’t get to hide a bad footnote.
(a) A previous draft cited a “2026 systematic review” (Carda-Navarro et al., Front Dent Med) as its central counter-evidence. That paper does not appear to exist. It was checked against PubMed and Crossref and could not be found. The author name and the journal are both real; the paper is not — which is precisely what a fabricated citation looks like. It has been removed. What replaced it — notes 2, 3, 4, 12 and 13 — is real, verified against PubMed by PMID, and says something stronger than the citation that was invented. A narrative review cited alongside it (Dasgupta & Rozario 2020) has been cut as well.
(b) A previous draft opened on the statistic that “71% of bruxers clenched on both sides at once,” attributed to note 1. That figure could not be verified in the cited paper, and it has been removed. The paper’s actual finding — that the splint does not stop the bruxing, and the wear returns in the same pattern — is both verifiable and a better opening, so it is now the opening. Every remaining number in this letter has been checked against its source, by PMID, one at a time.
(c) An earlier version described PRI’s clenching cascade as “documented” while simultaneously flagging it as an unvalidated framework claim. It can’t be both. That version also carried a population-level claim that foot posture and bite classification track together, resting on a single cross-sectional study of children whose own authors called it “insufficient to demonstrate a cause-effect relation.” Both the cascade-as-evidence framing and the foot-to-bite claim are gone, along with the study behind them. They were not load-bearing for the argument that remains — which is the point. The argument got stronger when they came out.
If any of this changed how you think about your own body, an assessment is where that conversation starts.