
Anxiety isn't only in your head.
The breath underneath the feeling
Breathing and anxiety are genuinely linked — but not the way you've been told. What the evidence supports, what it doesn't, and where our framework begins.
You’ve tried the apps. The guided meditations. The deep breaths. Maybe therapy, maybe medication. And maybe those things have helped — partially, or for a while.
Originally sent to AER members as an email. The exact send date wasn’t recovered — the date shown reflects publication order, not a precise record.
So here’s a question worth sitting with: what if some part of what you’re feeling isn’t starting in your thoughts at all — but in the way you’re moving air, right now, without noticing?
That question has a real answer, and it arrives in two halves. One half is well-documented physiology I can point you to. The other half is our clinical framework — a working model of why a person gets stuck breathing badly in the first place. Those are not the same kind of claim. Most of the internet will happily blur them together for you. I’d rather not.
I’m also going to correct two things you’ve almost certainly been told about breathing and anxiety, both of which are wrong.
The half that’s well established
Your breath and your nervous system aren’t neighbors. They’re wired together, cycle by cycle.
Your heart speeds up slightly as you inhale and slows as you exhale. That’s respiratory sinus arrhythmia, and it’s not subtle once you look for it. The mechanism is that the brainstem withholds vagus-nerve input to the heart during inhalation, then restores it on the exhale.1 The breath, in other words, is a gate — and what’s being gated is the parasympathetic brake.
Correction #1: inhaling does not “switch on” your fight-or-flight
You’ll read everywhere — including in an older version of this very letter, which is why I’m fixing it here — that inhalation activates the sympathetic nervous system. That’s mechanistically wrong.
Your heart rate rises on the inhale because the vagal brake is briefly lifted, not because a sympathetic surge fires.1 Sympathetic signaling is far too slow to produce a beat-to-beat change like that; it works on a timescale of seconds, not milliseconds. The correct sentence is: inhaling takes the brake off. Exhaling puts it back on. No adrenaline required.
It’s a small distinction, and it matters, because “every inhale is a little jolt of stress” is the kind of tidy story that leads people to strange places — like being faintly afraid of breathing in.
What actually helps: slow down
Here’s the finding that survives contact with the evidence. Slow breathing is associated with lower anxiety and lower arousal — while alertness holds.2 Calm and clear, rather than calm and dull. That’s worth having.
But the mechanism everyone assumes is behind it turns out not to be.
The honest status of “make your exhale twice as long”
Here’s where I have to be careful, because this is advice I give.
The theory is elegant: the exhale is the vagal phase, so a longer exhale should mean more brake.3 It’s a reasonable model, and it may well be right. But it is not settled, and I’d rather tell you that than sell you a certainty I don’t have.
The literature is genuinely split. Some studies find that lengthening the exhale, at a slow rate, does raise vagal tone.4 Others — including the largest and longest trial anyone has run, twelve weeks and a hundred people — find no difference at all between a long exhale and an even one.5 And a study of 828 people that randomised both the rate and the ratio found that rate predicted how much calmer people felt, cleanly and linearly, while the ratio predicted nothing.6 (That one measured how people said they felt, not their physiology — so it speaks to the feeling, not the vagus.)
What survives all of it: slowing down works. Around six breaths a minute is the number with real weight behind it. Whether the exhale needs to be longer than the inhale, on top of that, is an open question that honest researchers are still arguing about.
So if you’ve been dutifully counting 4-in, 8-out and feeling like you’re failing at the arithmetic — stop counting. Go slower. That’s the part the evidence is sure about.
I’m spelling this out rather than quietly teaching the ratio as fact, because you deserve to know which parts of what I tell you are load-bearing and which parts are a reasonable model still being tested.
And the exhale still matters enormously in our work — but the reason I care about it is mechanical, not autonomic. It’s about where your ribs end up, not about the vagus nerve. I’ll get to that, and I’ll label it clearly when I do.
The part that genuinely surprised me
Now the thread that runs straight at anxiety.
There’s a long-standing link between hyperventilation and panic. Not “panic makes you breathe fast” — everyone knows that. The other direction: chronically over-breathing, blowing off more carbon dioxide than your body is producing, appears to be part of what keeps the system primed. People with panic disorder tend to run low on CO₂ as a baseline state.7
Is that a cause? Honestly: contested. The review literature says the evidence for the competing theories is inconclusive, and I’m not going to pretend otherwise.7 But the therapeutic evidence runs in an interesting direction.
In one trial, patients with panic disorder — most of whom were already hypocapnic before anything happened — were taught a breathing therapy. Its goal was not what you’d guess.
The therapy did not teach big, deep breaths. It taught people to breathe less — slower, lighter, lower — in order to raise their carbon dioxide back into the normal range. Their CO₂ climbed from hypocapnic into the normal band, and panic measures improved substantially.8 In a later trial pitting breathing training against cognitive training, the change in CO₂ was the variable that statistically carried the improvement for the breathing group.9
Which means the advice you have received a thousand times — just take a nice deep breath — is, for some anxious people, a push in precisely the wrong direction. A big gulping inhale is more of the pattern, not less of it.
These are small trials, in panic disorder specifically, not in every flavor of anxiety. The limitations are real and I’ve listed them in the fine print rather than burying them. But the direction is consistent with everything above: less air, more slowly. Not more air, more deeply.
Try this now — 60 seconds
Breathe less, not more
Don’t take a big breath. That’s the whole trick.
Slow the rate down — that’s the part with evidence behind it. Aim for something like six breaths a minute: in for a count of about five, out for about five. Don’t chase a ratio; chase the slowness.
Breathe in through your nose, small and easy — less than feels natural. Then let the air out through your nose quietly and all the way, until your lower front ribs settle down and in. Pause a beat at the bottom, genuinely empty. Then let the next breath arrive on its own instead of pulling for it.
Six breaths, about a minute. If you notice a mild air-hunger, that’s expected — that’s your CO₂ coming back up, not something going wrong.
You didn’t calm yourself down. You stopped signaling emergency with every breath.

The half that’s our framework
Now the honest part, and the reason this letter isn’t just “breathe slower, good luck.”
Everything above establishes that a fast, over-breathing pattern travels with a revved-up nervous system. None of it explains why a particular person can’t stop breathing that way — even knowing all of this, even actively trying.
That’s the question our framework answers. And I need to be exact about what kind of answer it is.
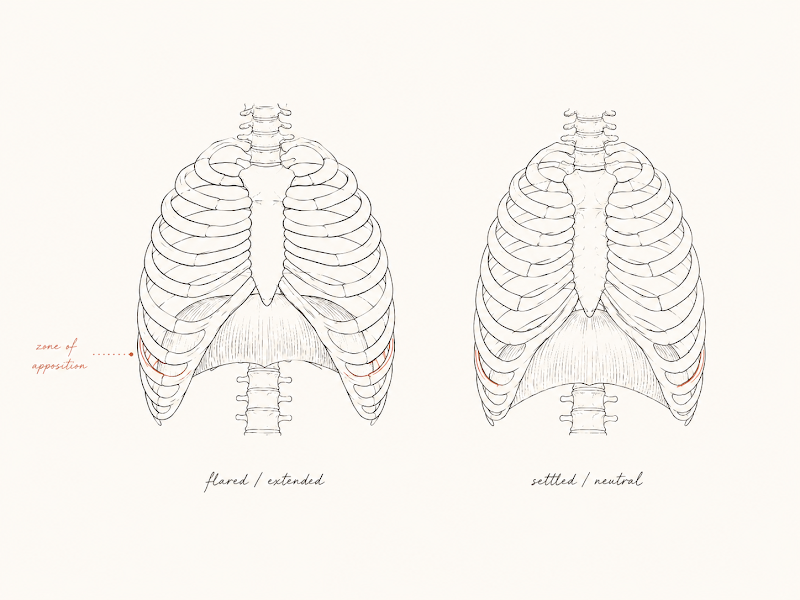
In the Postural Restoration model, the culprit is position. When the ribcage parks in a flared, expanded posture, the diaphragm flattens and loses its zone of apposition — the deep seal of contact against the rib wall that lets it fully ascend on the way out. Air still goes in fine. It’s getting it all out that quietly stops happening, and the neck and chest take over the job.† That’s why we care about the exhale: not as a calming ratio, but as the thing that restores the mechanics. I’ve written the full chain out at length — the whole mechanism is here — so I won’t re-teach it.
Read this line twice
That a flared ribcage causes or reinforces anxiety is our framework — not a finding from a peer-reviewed trial.†
Let me lay the chain out honestly, because it has four links: flared ribcage → flattened diaphragm and lost zone of apposition → an altered, inhale-dominant breathing pattern → anxiety.
Only the last link has real evidence behind it. Breathing pattern and anxiety are genuinely, physiologically connected — that’s citations 1 through 7. And ribcage position genuinely does change diaphragm mechanics; that’s ordinary respiratory physiology, not a fringe idea.
But no study has tested ribcage position against anxiety directly. Nobody has measured people’s rib position, restored it, and watched anxiety scores move. It hasn’t been done.
So: we think the model is right. We use it every day and we watch it work. And we’re telling you plainly that it is a working model, not a finding. Anyone who tells you “science says your ribs are making you anxious” is selling you something — and you should hold me to that same standard if I ever get sloppy about it.
What I’ll defend without hedging is the narrower claim underneath: if your structure can’t finish an exhale, then being told to breathe slower is you fighting your own mechanics. You can override it for sixty seconds — you probably just did. Making it your default is a different problem, and we think it’s a positional one.†

Does any of this sound like you?
Not a diagnostic checklist — there’s no score at the bottom. Just what people tend to describe on the way in the door:
- Chest tightness or pressure that’s already been cleared as non-cardiac
- Never quite getting a satisfying deep breath, no matter how hard you pull for one
- Jaw clenching or grinding, especially at night
- Shoulders that won’t drop no matter how much you stretch them
- A persistent “wired but tired” hum
- Racing thoughts that get louder the moment you lie down
If you recognized yourself in that list, the useful next move isn’t to breathe harder. It’s to find out whether your body is physically organized in a way that permits rest at all.
The necessary caveat, and I mean it
This does not replace mental health care. Not as a legal formality — as a fact about scope.
If you’re managing clinical anxiety, panic, or anything in that neighborhood, this work is meant to sit alongside qualified mental-health treatment, never instead of it. I’m not a psychologist, and this isn’t therapy. We address one contributing factor — the mechanical and respiratory environment that can make it harder for a nervous system to find its way down. There are many others, and some of them need a clinician, a diagnosis, or medication. Anxiety that is severe, worsening, or new deserves a proper workup. Nothing here is medical advice.
Where this leaves you
The breathing–anxiety link is real and well documented. Slowing down is the part with evidence under it. The exhale-ratio rule you’ve been counting out is not, and I’d rather hand you the correction than the folklore.
Whether your breath is being blocked by your structure — and what to do about it if it is — is a question about you specifically. That’s what an assessment is for.
Neutrality first. Then build.

The fine print
-
Eckberg DL. The human respiratory gate. J Physiol. 2003;548(Pt 2):339–352. Respiration phasically modulates the responsiveness of vagal cardiac motoneurones — the brainstem withholds vagal outflow during inspiration and restores it in expiration, producing respiratory sinus arrhythmia; heart-period lengthening begins in early expiration. Limitation: this is normal cardiorespiratory physiology in healthy people. It establishes that breath phase gates vagal outflow — not that changing how you breathe treats an anxiety disorder. It is also the basis for the correction above: the beat-to-beat rise in heart rate on inhalation reflects vagal withdrawal, not sympathetic activation, which operates far too slowly to account for it.
-
Zaccaro A, et al. How breath-control can change your life: a systematic review on psycho-physiological correlates of slow breathing. Front Hum Neurosci. 2018;12:353. Slow breathing is associated with increased vagally-mediated HRV and with greater alertness alongside reduced arousal and anxiety. Limitation: despite the title, this functions as a narrative review rather than a meta-analysis — roughly 15 studies, no randomized controlled trials among them, and healthy participants only. Effects are largely acute (measured during or just after practice), not demonstrated durable shifts in resting baseline, and outcomes lean heavily on self-report.
-
Gerritsen RJS, Band GPH. Breath of Life: the respiratory vagal stimulation model of contemplative activity. Front Hum Neurosci. 2018;12:397. Proposes that slow breathing — and longer exhalations specifically — stimulates the vagus nerve. Limitation: this is a theoretical model synthesizing existing work, not a controlled trial. It is cited here to show where the popular “long exhale” rule comes from. The empirical tests of the rule run both ways — citation 4 finds a vagal advantage for the longer exhale; citations 5 and 6 do not — so we present the model as the model it is: well-motivated, and contested.
-
Van Diest I, Verstappen K, Aubert AE, Widjaja D, Vansteenwegen D, Vlemincx E. Inhalation/exhalation ratio modulates the effect of slow breathing on heart rate variability and relaxation. Appl Psychophysiol Biofeedback. 2014;39(3–4):171–180. Thirty participants breathed at 6 or 12 breaths/min with an inhale:exhale ratio of 0.42 or 2.33. A longer exhale produced greater high-frequency HRV — but only at the slow rate. Also greater self-reported relaxation. See also Laborde S, et al. Slow-paced breathing: influence of inhalation/exhalation ratio and of respiratory pauses on cardiac vagal activity. Sustainability. 2021;13(14):7775 — 64 athletes at 6 cycles/min; longer exhalation produced higher vagally-mediated HRV (RMSSD). Limitation: both are small, acute, healthy-participant laboratory studies measuring HRV during or immediately after the breathing itself — not durable change, and not clinical anxiety outcomes. Note the interaction in Van Diest: the ratio only mattered once the rate was already slow.
-
Birdee G, Nelson K, Wallston K, Nian H, Diedrich A, Paranjape S, Abraham R, Gamboa A. Slow breathing for reducing stress: the effect of extending exhale. Complement Ther Med. 2023;73:102937. A 12-week single-blind randomized controlled trial, n=100, comparing extended-exhale slow breathing against slow breathing with an equal inhale:exhale ratio, with HRV spectral analysis and PROMIS Anxiety as co-primary outcomes. Extending the exhale did not significantly outperform an even ratio. This is the largest and longest trial on the question, and it is null — which is why we describe the long-exhale rule as contested rather than established. The authors also note that slow breathing reduced psychological but not physiological stress as measured by HRV, which is itself worth sitting with.
-
Czub M, et al. A slow diaphragmatic breathing intervention for anxiety: how do respiration rate and inhalation/exhalation ratio influence self-reported anxiety? Stress Health. 2024;40(6):e3496. 828 participants (Poland and Spain) completed a 10-minute guided breathing exercise with respiration rate randomly sampled from 6–12 breaths/min and inhalation/exhalation ratio sampled continuously. Slower respiration rates were linearly associated with lower post-exercise anxiety; regarding the ratio, the authors state: “No significant relationships between inhalation/exhalation ratio and post-test anxiety level were found” — including when non-linear relationships were tested. Limitation, and it is a serious one: this study measured self-reported anxiety only. It recorded no physiology whatsoever — no HRV, no vagal measure. It is evidence that the ratio did not change how anxious people said they felt after a single online session. It is not evidence about the vagus nerve, and it does not by itself refute the long-exhale model.
-
Meuret AE, Ritz T. Hyperventilation in panic disorder and asthma: empirical evidence and clinical strategies. Int J Psychophysiol. 2010;78(1):68–79. A review: observational, experimental, and therapeutic findings together suggest an important role for low CO₂ in panic disorder. See also Boulding R, Stacey R, Niven R, Fowler SJ. Dysfunctional breathing: a review of the literature and proposal for classification. Eur Respir Rev. 2016;25(141):287–294, which reports clinically significant anxiety in 56% of people with dysfunctional breathing against 24% of well-controlled asthmatics. Limitation — stated by the authors of both, and important: the evidence for the competing causal theories is inconclusive. Boulding puts it plainly — “it is difficult to assess whether [hyperventilation syndrome] is causative or simply a secondary effect of anxiety related disorders” — and it is a narrative review, not a systematic one. Low CO₂ and disordered breathing are reliably observed alongside anxiety; that they cause it is not established. We present this as an association with suggestive therapeutic support, not as settled causation. It is, however, the reason we will not say “there is no evidence connecting breathing and anxiety” — that would be false in the other direction. The adjacent links are real. It is the specific chain from rib position to anxiety that nobody has tested.
-
Meuret AE, Wilhelm FH, Ritz T, Roth WT. Feedback of end-tidal pCO₂ as a therapeutic approach for panic disorder. J Psychiatr Res. 2008;42(7):560–568. Thirty-seven patients with panic disorder were randomized to capnometry-assisted breathing training or a delayed-treatment control; most (n=26) were hypocapnic at baseline, and mean pCO₂ rose from the hypocapnic range into the normal range across treatment, alongside large improvements on panic measures. Limitations, stated by the authors themselves: no active or placebo control condition, entirely uncontrolled long-term follow-up, and a small sample. It is also specific to panic disorder — do not read it as evidence about anxiety in general.
-
Meuret AE, Rosenfield D, Seidel A, Bhaskara L, Hofmann SG. Respiratory and cognitive mediators of treatment change in panic disorder: evidence for intervention specificity. J Consult Clin Psychol. 2010;78(5):691–704. Forty-one patients with panic disorder were randomized to respiratory training or cognitive training; change in end-tidal CO₂ mediated improvement in the respiratory arm, while threat appraisal mediated improvement in the cognitive arm. Limitation: small sample, and statistical mediation is evidence consistent with a causal path — not proof of one.
If any of this changed how you think about your own body, an assessment is where that conversation starts.