
You don't have a swing problem.
You have a rib cage full of air
You have a rotation problem — and rotation is a breathing problem. The turn you keep stretching for is waiting behind one full exhale.
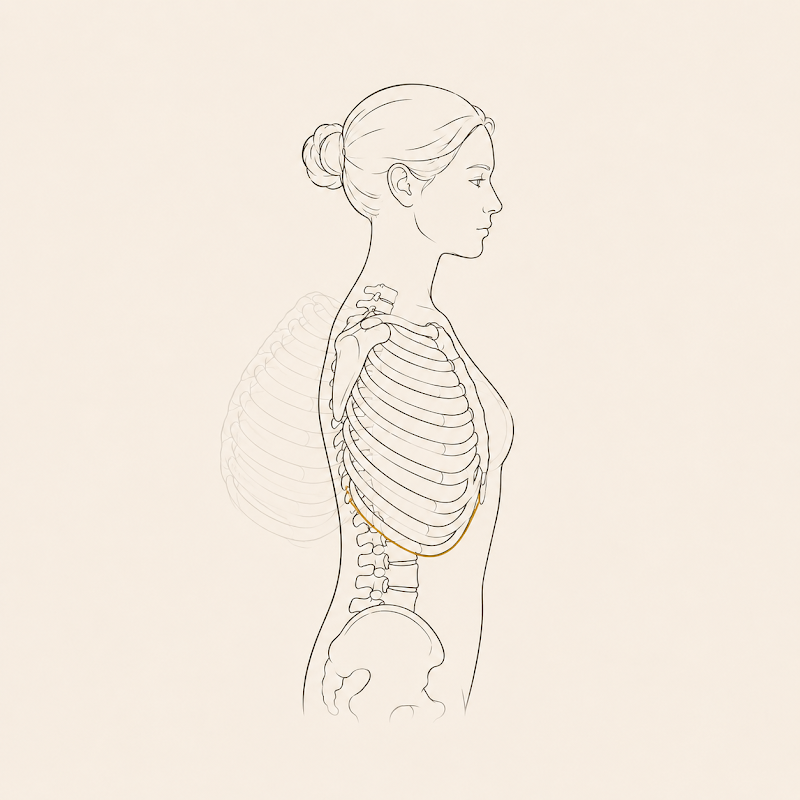
You’ve stretched. You’ve rolled the mid-back on a foam roller until it hurt. You’ve done the thoracic-mobility drills the internet sold you, and your backswing is still short on one side. Here’s the thing nobody told you: a rib cage that’s full of air can’t turn. Not won’t — can’t.
Originally sent to AER members as an email. The exact send date wasn’t recovered — the date shown reflects publication order, not a precise record.
Try this — 45 seconds
Find the turn you’re guarding
- Sit tall, feet flat. Cross your arms — right hand to left shoulder, left hand to right shoulder — and lift your elbows to about chest height. Let your head settle directly over where your forearms cross. (Locking your arms to your rib cage means you measure your real turn, not your reach.)
- Without forcing, rotate your whole trunk to the right as far as is comfortable. Let the elbows point the way, and clock where they aim — a spot on the wall, the edge of a doorway. Back to center. Now rotate left. Notice which side turns further, and how much effort each one costs.
- Drop your hands into your lap and exhale all the way out — slow, until the ribs come down and the belly draws in. Pause at the bottom, fully empty. Take two quiet breaths while keeping the ribs down — don’t let the chest pop back up.
- Re-cross the arms, elbows high, head centered, and turn to the harder side again.
For most people the elbows now point further around, with noticeably less effort. You didn’t stretch anything. You changed the position of your rib cage — and your rotation followed.

Why the turn stalls
A golf swing isn’t a shoulder move or a hip move you can isolate. It’s your whole trunk rotating one side against the other, and that turn requires your rib cage to compress and re-orient as it goes — ribs on one side drawing down and in while the other side opens.
Here’s the catch. An inflated rib cage can’t twist.† If you live chest-up and air-trapped — ribs flared, breath parked high — the cage is held open like a barrel pumped full of air, and it’s already wound slightly toward one side. You feel that as a backswing that’s short, blocked, or lopsided, and you go hunting for more mobility. The mobility was never missing. The air was never leaving.
The position underneath all of this — ribs down, diaphragm reseated against the lower rib cage, what’s called the zone of apposition — is the same one I’ve written about at length in Why you crash at 3 o’clock, and I won’t repeat the whole mechanism here. The short version, and it’s a confident one: rib cage position genuinely governs how well the diaphragm can work. The zone of apposition is where the diaphragm lies flat against your lower ribs and actually transmits force through them,1 and when a chest is held inflated, that zone measurably collapses — in severe hyperinflation it drops to roughly half its normal surface area.2 That’s not a theory. That’s mechanics.
What’s my extension is applying it to you.† That measurement was taken in diseased, hyperinflated lungs — not in a healthy golfer with a flared rib cage. That your chest-up posture costs you a slice of the same leverage, on the same mechanical logic, is the Postural Restoration framework’s inference. I think it’s a good one. It is still an inference, and I’ll mark it as one every time.
What’s actually happening
Your breathing muscle is also your rotation muscle
1. The diaphragm has two jobs. It’s your main breathing muscle and a core stabilizer. Dynamic MRI shows it actively working to control the trunk during limb loading, not just to move air.3 The same muscle that breathes you is part of how you organize a turn.
2. So do the muscles that turn you. The deep abdominals — transversus abdominis and the obliques that brace and rotate your trunk — pull double duty in breathing, and the very timing of when they fire shifts with what your breath is doing.4 Spend them on breathing and they aren’t free to organize your turn.
3. The two jobs compete. When breathing demand climbs — exertion, stress, or a chest-up posture that leaves you slightly air-hungry — the diaphragm’s postural contribution measurably drops.5 A system busy breathing can’t fully spend that same muscle on bracing and rotating. Empty the air first, and you free it for the turn.
4. Posture sets a ceiling on rotation. In older adults with neck pain, a more rounded thorax and a more forward head measurably reduced how far the neck could turn.6 That was measured at the neck, in one population — I’m extending the principle to the thorax, and I’ll say plainly that the extension is mine, not the study’s. But the logic is the same: the position you hold all day sets the rotation you get to use on the course.

Where this meets the method
You already know your body isn’t symmetrical — you can feel it in the cross-arm test. In the postural-restoration model there’s a structural reason for that, starting with a diaphragm that isn’t the same on both sides; I’ve laid that out in what PRI actually restores, so here it’s enough to say: the asymmetry is normal and expected.†
What isn’t normal is when it stops alternating. In this model, trunk rotation depends on the rib cage’s ability to internally rotate on one side — ribs drawing down and in — which is what a complete exhale delivers.† Lose the exhale and you lose that side’s ability to close, and the turn in that direction goes with it. For a lot of right-handed players, the direction that gets stiff is the backswing. Even out the rib position and the “good side / fighting side” gap starts to close.
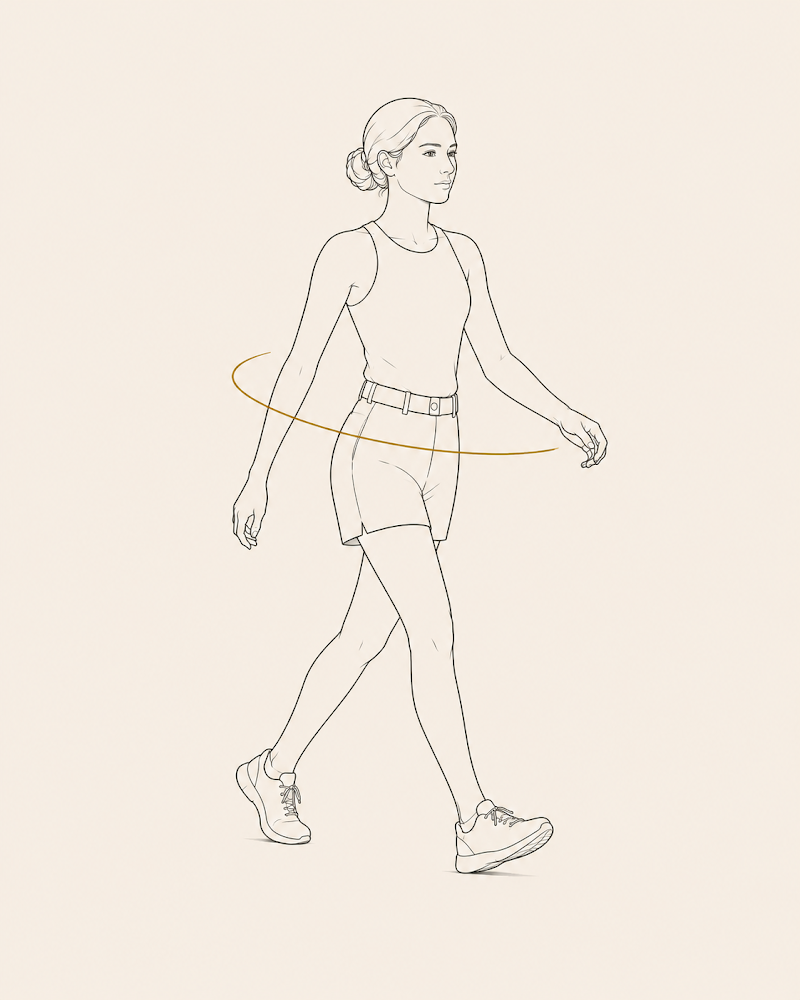
And the turn itself is reciprocal — one side opposing the other, the same alternating mechanism you use to walk. So we work the breath and the rib position first, then the rotation, because in this framework rotation is downstream of the air.†

A case in point
A representative composite — the pattern and the sequence are typical of what walks in; the person is not one client.
A right-handed golfer, frustrated: the backswing feels short and stuck, and months of stretching and rolling the mid-back haven’t moved it. The cross-arm test tells the story in fifteen seconds — he turns easily to the left, fights the turn to the right, and the moment he exhales completely, the stuck side opens. The rib cage is sitting full and flared. The turn isn’t missing. It’s locked behind air he never lets out.†
| Step | What we do |
|---|---|
| 1. Reposition with the breath | A reach on a long, full exhale draws the lower ribs down and in and re-orients the spine — restoring the zone of apposition on the side that couldn’t close, so the trunk can rotate that way again.† |
| 2. Own it with the deep abdominals | A position he can’t hold isn’t his yet. We hold the new rib position with the internal obliques and transversus abdominis — whose activity is already wired to the breath4 — so the shape survives when the reach comes off, not only while he’s pulling on something.† |
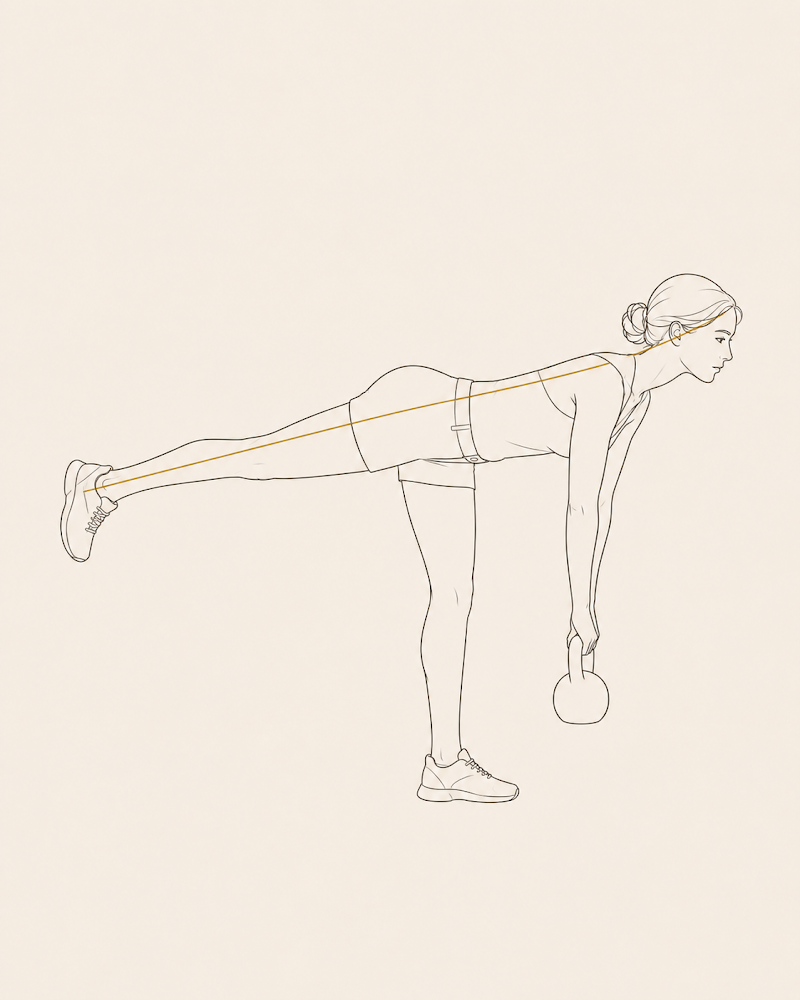
| 3. Rotate into it | Now he turns — reciprocal, one side against the other, in a staggered stance — physically rotating the trunk while those deep abdominals keep the ribs from springing back open. The turn re-learned, not stretched.† |
| 4. Load it | Then we add load and speed, so the new rotation holds at the force of an actual swing — not just on the mat.† |
In the room, a blocked backswing typically moves more freely and with less effort inside the first session — that part is immediate, and you feel it. What takes weeks is the loading. That’s what makes the new turn hold on the course instead of slipping back by the next round.
I won’t tell you how many degrees you’ll gain. I don’t know, and neither does anyone who promises you a number they haven’t measured on you.
Why it matters past the tee
This isn’t only golf. Every rotational athlete — the swing, the throw, the change of direction — and every lifter who needs a braced trunk under load runs on the same rule: power comes from rotating through a trunk you can stabilize and breathe in at the same time. Chase mobility and you’ll stretch forever. Restore the rib position and the rotation you were missing simply shows up.
And under the bar it compounds. The same full exhale that frees the turn is the one that lets you brace and load it — which is exactly where strength gets built.
We test this in the first session. You’ll see which way you rotate, change it with your own breath, and feel the difference before you leave the room.
— Peter Jang, MFA CSCS PRT AER on Newbury · Certified Postural Restoration Center
The fine print
-
De Troyer A, Wilson TA. Action of the diaphragm on the rib cage. J Appl Physiol. 2016;121(2):391–400 — describes the “appositional force,” by which abdominal pressure is transmitted to the lower rib cage through the zone of apposition. This is settled mechanics. The zone of apposition is real, and it is load-bearing.
-
Cassart M, Pettiaux N, Gevenois PA, Paiva M, Estenne M. Effect of chronic hyperinflation on diaphragm length and surface area. Am J Respir Crit Care Med. 1997;156(2):504–508 — 3D reconstruction from spiral CT found the zone-of-apposition surface area reduced to about 54% of normal in hyperinflated patients, while the dome surface area was unaffected. Limitation, and it matters: 10 patients with severe COPD versus 10 controls. This is pathological hyperinflation of diseased lungs. It proves that rib cage inflation governs the zone of apposition. It does NOT prove that a healthy golfer’s flared rib cage does the same thing to a meaningful degree — that extension is the framework’s, and it is marked † in the text. (The same physiology underwrites Hoover’s sign, a validated clinical finding in hyperinflation.)
-
Kolar P, Sulc J, Kyncl M, et al. Stabilizing function of the diaphragm: dynamic MRI and synchronized spirometric assessment. J Appl Physiol. 2010;109(4):1064–1071 — in 30 healthy subjects, diaphragm excursion during isometric limb loading exceeded that of tidal breathing, evidencing a postural role alongside the respiratory one. Limitation: 30 subjects, supine, isometric limb tasks against resistance. It establishes the diaphragm’s dual role; it does not study rotation, and it does not study golf.
-
Hodges PW, Gandevia SC, Richardson CA. Contractions of specific abdominal muscles in postural tasks are affected by respiratory maneuvers. J Appl Physiol. 1997;83(3):753–760 — postural activity of the deep abdominals, transversus abdominis included, is modulated by breathing. Limitation: a small laboratory study of arm-movement tasks. It grounds the breath–deep-abdominal coupling, not the training sequence built on top of it.
-
Hodges PW, Heijnen I, Gandevia SC. Postural activity of the diaphragm is reduced in humans when respiratory demand increases. J Physiol. 2001;537(3):999–1008. Limitation: respiratory demand was raised experimentally in the lab (increased CO₂ and dead space), not by posture. That a chest-up posture raises breathing demand the same way is my inference from the framework, not this study’s finding.
-
Quek J, Pua YH, Clark RA, Bryant AL. Effects of thoracic kyphosis and forward head posture on cervical range of motion in older adults. Man Ther. 2013;18(1):65–71. Limitation: cross-sectional, 51 older adults with cervical spine dysfunction, and the rotation measured was at the neck. The application to thoracic and trunk rotation is stated in the text as my extension, not the paper’s conclusion.
A note on what this letter does not claim: nothing here rests on the idea that a longer exhale is autonomically superior to simply breathing slowly — a question the evidence has not settled. The exhale earns its place here on mechanical grounds (notes 1 and 2): it is what brings the ribs down. That is a separate argument from the calming one, and it is the one I’m making.
This is educational, not medical advice. If you have pain, a disc or rib injury, or you’re pregnant, check with a qualified clinician before changing how you breathe or rotate under load.
If any of this changed how you think about your own body, an assessment is where that conversation starts.