
What PRI actually restores.
The pattern behind the symptoms
The back that keeps going out. The hip that clicks. The neck that needs to crack. One pattern underneath — and one place to work.
Your left side isn’t missing. You use it every day. But your brain’s sense of it may be quietly fading — and a surprising number of things you’ve been treating as separate problems sit downstream of that one fact.
Originally sent to AER members as an email. The exact send date wasn’t recovered — the date shown reflects publication order, not a precise record.
You are not built evenly
Open any anatomy text and you’ll find the same thing. Your right hemidiaphragm sits higher than the left, and underneath it is the liver — a dense, solid organ that gives that side of your breathing muscle something to press against. The left has no such foundation. Under it sits the stomach: gas, fluid, and not much resistance. Meanwhile the heart sits left of center, and the left lung gives up a lobe to make room for it — three on the right, two on the left.1
None of that is a defect. It’s just how a human is assembled, and every human is assembled that way.
Here’s where I want to be precise, because this is exactly the point where writing about this stuff usually goes soft. Everything in the paragraph above is textbook anatomy. What Postural Restoration adds is a clinical model built on top of it: that this built-in asymmetry gives you a default lean — a tendency to settle into the right side, push off the right, breathe more effectively on the right — and that a healthy system cancels that tendency out through alternation.† Left, then right. Stance, then swing. One side loads while the other lets go, thousands of times a day, and the asymmetry never gets a chance to become a position.
Stop alternating, though, and it does. The right side does more, so it gets better at doing more. The left side does less, so the brain gets less information back from it, so it does less still. That’s the whole engine, and it’s not exotic: it’s just what happens to any system that stops using half of itself.
The symptoms are one symptom
You already know the list. The low back that keeps going out. The hip that clicks on one side. The shoulder that won’t stay fixed no matter how many times somebody fixes it. The neck that needs to crack every single morning.
Treated separately, these look like four problems. Treated as a group, they start to look like four reports from one problem.
That instinct isn’t unique to PRI, and it isn’t fringe. The broader musculoskeletal literature has a name for it — regional interdependence — and a real evidence base: treat the hip and knee pain improves; treat the thoracic spine and neck symptoms improve. Distant regions demonstrably talk to each other.2 That much is established.
What’s not established — and I’ll say it plainly — is the stronger claim that every one of those symptoms traces back to a single, describable postural pattern. That’s PRI’s clinical model.† It’s a coherent one, it’s been refined over decades of clinical work, and it’s the one I’ve found most useful. It is not a finding from a trial.
The pattern isn’t really in the muscles
Here’s the part that took me longest to understand, and it’s the part that actually matters.
When a side of you goes quiet — when the brain stops getting clean, high-resolution information back from it — the brain doesn’t just shrug and accept the loss. It compensates. It builds patterned behavior to keep operating a limb it can no longer fully feel: extra tension here, a substituted muscle there, a rotation that borrows range from somewhere it shouldn’t.
Think of it as scaffolding. And the scaffolding works — that’s the whole problem with it. You stay upright. You keep training. You get through your day. But it’s a structure holding up a building, not the building.
And scaffolding has a cost, because it feeds itself. It substitutes for real sensation, which means the real sensation gets used less, which means it fades further, which means the scaffolding becomes more load-bearing. Round and round. The brain ends up piloting a body it’s partly guessing about.
(The scaffolding image is mine — a metaphor for the compensatory process, not a structure anyone has found on a scan.)
Why a body problem starts acting like a mood problem
Now the part people don’t expect.
A brain running a body it can’t fully feel is a brain that has to stay a little more vigilant. Not metaphorically — the systems that track where your body is and the systems that decide how threatened you are are neighbors, and they share wiring. In the neuroimaging literature, weakened communication between the prefrontal cortex and the amygdala travels with a heightened, more easily-tripped threat response.3
So you get the person who startles at sounds that never used to register. Who carries a low, sourceless hum of anxiety. Whose ground just feels a little less solid than it should — not because anything is actually wrong in the room, but because the system doing the threat math is working from incomplete information about its own body.
I want to be careful here, because this is a correlation, not a chain of proof. That the brain-body map and the threat response are linked is well supported. That your postural pattern is what dimmed your map is a clinical read, not a lab result.†
A popular claim, corrected
You’ve probably heard some version of: “your brain can’t tell the difference between physical and psychological stress.” It’s a great line. It’s also not true, and it’s worth fixing, because the truth is more useful.
Your brain absolutely tells the difference. Physical stressors — blood loss, low blood sugar, pain — take a fast, reflexive brainstem route in. Psychological ones — the email, the deadline, the conversation — have to be appraised first by the limbic forebrain. Researchers can even dissociate them: knock out one ascending pathway and you blunt the response to physical stressors while leaving the psychological ones intact.4
Here’s the part that’s true, and it’s the part that actually matters: they converge. Different routes in, same machinery out — the HPA axis, the sympathetic nervous system. Cortisol, heart rate, breathing rate, muscle tone. Your body pays in the same currency no matter which door the stress came through.
Which is the real point: it’s the total load that has to add up, not just the athletic part of it. A hard week and a hard workout draw on the same account.
Try this now — 60 seconds
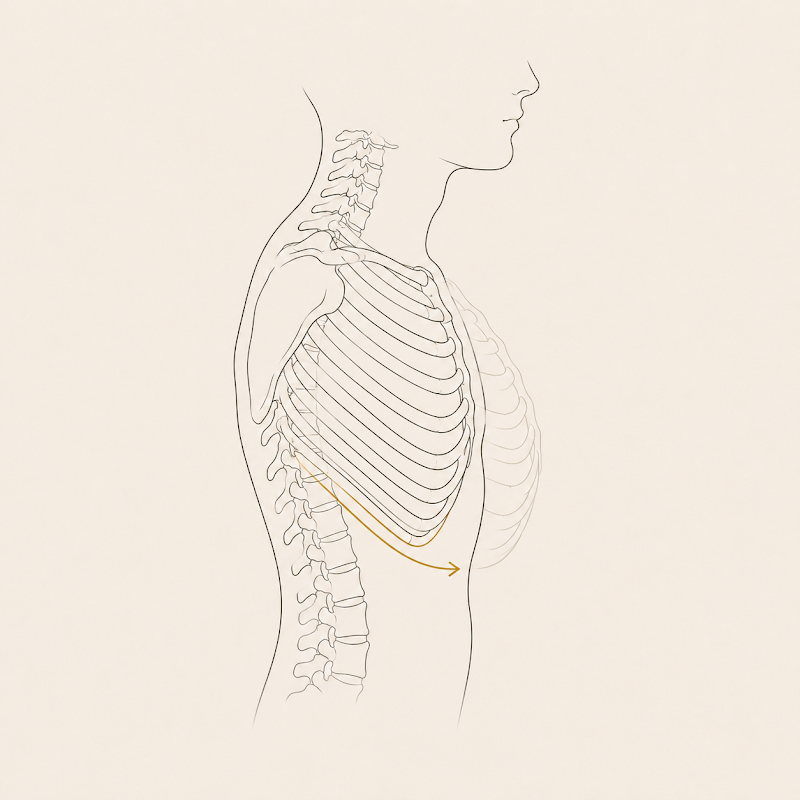
Find the floor
Sit back. Breathe in through your nose, easy — don’t gulp at it. Now breathe out slowly and all the way, letting the exhale run about twice as long as the inhale, until your lower front ribs settle down and in. Pause a beat at the bottom, completely empty. Let the next breath arrive on its own rather than reaching for it.
Six breaths. About a minute.
Notice what changed. Not your muscles — your volume. The floor got a little more solid, the room got a little less loud.
That’s not relaxation. That’s your nervous system getting better information and deciding it can stand down.
(Why the exhale specifically, and what it does to the rib cage, is the whole subject of Why you crash at 3 o’clock.)

What PRI restores, in order
The order is not decorative. It’s the method.†
First: the breath. It’s the only direct line you have.
Respiration is the one autonomic function you get a vote in. You can’t consciously lower your cortisol or dilate a blood vessel, but you can change how you breathe — and the breath is wired straight into the arousal system. Slowing the rate down — toward six breaths a minute — reliably raises heart-rate variability and tips the balance toward the recovery side of the nervous system.5
That’s why we start here and not with a stretch. Nothing downstream holds while the system is still running hot.
Then: the structure the brain lost track of
With the nervous system quieter, the actual work can start — and PRI runs it in a specific sequence: pelvis, then thorax, then the shoulder girdle, then cervical, then cranial. Ground up.†
This is the low back that finally stops going out — not because I treated the back, but because the pelvis that was driving the rotation stopped driving it. The hip that clicked because the femur was sitting badly in its socket stops clicking when the socket moves. The scaffolding comes down because the building can stand.
Then: the senses
For a lot of people the compensation never stopped at structure. The brain adapted its inputs too.
How do you feel stable when your structure has shifted? You lock the neck — and neck proprioception is not a minor player. Disturbed sensory signaling from the cervical spine is associated with dizziness and impaired balance and spatial orientation.6 How do you find yourself in space when your foundation has moved? You narrow your visual focus and lean on the sense you trust most.†
And vision isn’t just for seeing. There’s a whole visual stream — the dorsal stream — whose job is not perception at all but the moment-to-moment guidance of movement.7 Your eyes are part of your motor system. So is your bite. So is the pressure under your feet.
Which is why the last piece of this work happens from the neck up, and why it’s the piece that finally lets people let go.
Why PRI, and my honest hedge
I get asked this a lot, so: is PRI the only thing that works?
No. Obviously not. Plenty of excellent practitioners get excellent results with other models, and anyone who tells you their system is the only real one is selling you something.
Here’s the true version of why I use it. I’ve trained across a lot of systems, and PRI is the most complete one I’ve found — not the only good one, but unusually thorough in scope: it starts at assessment, gives you an actual sequence, and carries all the way through to what you do about it, including the parts most systems drop on the floor (the breath, the eyes, the bite). That’s my judgment after years of using it, offered as a judgment — not as a fact about the field.
Two more things, said straight:
It’s a small world. There are only about seventy practitioners in the United States holding the full PRT credential. That’s a real scarcity, and it’s why people fly in. It’s also not a magic certificate — it’s a credential, and credentials describe training, not outcomes.
It is not medicine. I’m a movement specialist, not a physician. PRI doesn’t treat disease, and I don’t. What it does is restore the sensory and structural integrity that lets a body perform, recover, and adapt without fighting itself — which is a real thing, and a different thing.
Why this reaches past pain
Here’s one thread that surprises people, and it’s a good test case for how to hold this kind of claim honestly.
Your mouth is part of your motor system. That’s not a metaphor. The ligaments suspending each tooth in its socket are packed with mechanoreceptors that encode how hard you’re biting and in what direction, and those signals feed directly into the fine motor control of the jaw. Pull the teeth out and you lose the sensor, and the motor control degrades with it.8 The bite is an input.
Now the part where I have to be careful with you. Across fourteen longitudinal studies pooled together, tooth loss is associated with cognitive impairment and dementia — and in a dose-dependent way: more teeth lost, higher risk.9
And that association is almost certainly not a clean causal story. Tooth loss is one of the most socioeconomically loaded variables in all of epidemiology — it travels with poverty, less education, smoking, diabetes, poor nutrition, and worse access to care. Reverse causality is live, too: early, still-invisible cognitive decline degrades a person’s self-care, including how well they brush. And no trial has ever shown that restoring chewing prevents dementia.
So what do you do with that? You hold it as what it is: a real, dose-dependent, repeatedly-replicated signal that is not a proven mechanism. Interesting enough to take seriously. Not strong enough to sell anybody anything. That’s the whole discipline of this, and if I ever hand you one of these without the other half, you should stop trusting me.
What it does support — modestly, and this is the version I’ll defend — is the design principle: the mouth, the eyes, the feet and the diaphragm are all feeding the same brain, and a model that ignores three of them is working with less than it could.

Is this you
If you’ve been treating the back, the hip, the shoulder, the neck — one at a time, for years — and they keep coming back, then the thing nobody has addressed may be the thing connecting them.
And if you have the nagging sense that your body has more in it than you can currently get to: that may not be a problem with your body at all. It may be a problem with your brain’s map of it.
Maps can be redrawn.
The fine print
-
Diaphragmatic and thoracic asymmetry — the right hemidiaphragm sits higher, supported inferiorly by the liver; the left lung has two lobes to the right lung’s three, accommodating the heart. Standard descriptive anatomy (Gray’s Anatomy, 42nd ed., 2020). Limitation: none — the anatomy isn’t in dispute. What’s inferred FROM it below (that this produces a predictable postural pattern) is the framework claim, not the anatomy.
-
Wainner RS, Whitman JM, Cleland JA, Flynn TW. Regional interdependence: a musculoskeletal examination model whose time has come. J Orthop Sports Phys Ther. 2007;37(11):658–660; Sueki DG, Cleland JA, Wainner RS. A regional interdependence model of musculoskeletal dysfunction. J Man Manip Ther. 2013;21(2):90–102. Supporting trials include hip treatment improving knee symptoms and thoracic treatment improving cervical symptoms. Limitation: regional interdependence establishes that distant regions influence each other — it does NOT establish that a specific list of symptoms all arise from one underlying postural pattern. That further step is PRI’s clinical model, marked † above.
-
Kim MJ, et al. The structural and functional connectivity of the amygdala: from normal emotion to pathological anxiety. Behav Brain Res / Dialogues Clin Neurosci. 2011;13(4):403–418; Etkin A, Wager TD. Functional neuroimaging of anxiety: a meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. Am J Psychiatry. 2007;164(10):1476–1488. Limitation: this is associational neuroimaging in anxiety populations. It shows that weakened prefrontal–amygdala connectivity travels with a heightened threat response. It does NOT show that losing proprioceptive awareness of a body region causes that state — that direction of causation is a clinical inference, and is marked † in the text.
-
Ulrich-Lai YM, Herman JP. Neural regulation of endocrine and autonomic stress responses. Nat Rev Neurosci. 2009;10(6):397–409. Systemic/physiological stressors engage reflexive brainstem pathways; psychogenic stressors require limbic forebrain appraisal — a dissociation demonstrated by lesion work — but both converge on shared HPA-axis and sympathetic output. Limitation: much of the pathway-level dissociation comes from rodent lesion studies; the convergence downstream is the well-supported part, and it’s the part the text relies on.
-
Russo MA, Santarelli DM, O’Rourke D. The physiological effects of slow breathing in the healthy human. Breathe. 2017;13(4):298–309; Zaccaro A, et al. How breath-control can change your life: a systematic review on psycho-physiological correlates of slow breathing. Front Hum Neurosci. 2018;12:353. Limitation: the reviews’ own authors note the evidence base needs strengthening and the underlying studies are heterogeneous. The reliable finding is an acute effect during and shortly after practice — not a guaranteed shift in your all-day baseline.
A second, narrower point, since the practice above asks you to lengthen the exhale: the well-established lever is the slow rate. Whether a longer exhale adds anything on top of the slow rate is genuinely unsettled. There’s a proposed vagal mechanism for it (Gerritsen RJS, Band GPH. Breath of life: the respiratory vagal stimulation model of contemplative activity. Front Hum Neurosci. 2018;12:397) and several trials finding an advantage — but the largest head-to-head test found none: Birdee G, et al. Slow breathing for reducing stress: the effect of extending exhale. Complement Ther Med. 2023;73:102937 — a 12-week RCT (n=100) comparing exhale-longer-than-inhale against exhale-equals-inhale, which found no significant HRV difference between them. Contested, not settled. I still teach the long exhale, for reasons that are structural rather than autonomic — see Why you crash at 3 o’clock — but I’m not going to tell you the ratio is a proven autonomic lever when the best trial says otherwise.
-
Kristjansson E, Treleaven J. Sensorimotor function and dizziness in neck pain: implications for assessment and management. J Orthop Sports Phys Ther. 2009;39(5):364–377. Limitation: a clinical review; the association between disturbed cervical sensory input and impaired balance/orientation is well described in neck-pain populations, but this does not establish that “locking the neck” is a deliberate compensation for a postural pattern — that reading is framework.
-
Goodale MA, Milner AD. Separate visual pathways for perception and action. Trends Neurosci. 1992;15(1):20–25. The dorsal stream converts vision into motor control rather than conscious perception. Limitation — and this one matters: this paper is about visual neuroscience. It supports exactly one claim here — that vision is part of the motor system. It says nothing about gait, respiration, or postural patterns, and I’m not citing it for any of those.
-
Trulsson M. Sensory-motor function of human periodontal mechanoreceptors. J Oral Rehabil. 2006;33(4):262–273. Periodontal receptors encode the amplitude and direction of tooth loads and feed the fine motor control of the jaw; these sensory-motor functions are lost or impaired when teeth are extracted. Limitation: a review of microneurography work in small samples, and it’s about jaw motor control specifically — not about whole-body posture.
-
Qi X, Zhu Z, Plassman BL, Wu B. Dose-response meta-analysis on tooth loss with the risk of cognitive impairment and dementia. J Am Med Dir Assoc. 2021;22(10):2039–2045. Fourteen longitudinal studies, 34,074 participants: more tooth loss was associated with cognitive impairment (pooled RR 1.48, 95% CI 1.18–1.87) and dementia (RR 1.28, 95% CI 1.09–1.49), dose-dependently. Limitation — stated by the authors themselves: observational only. Tooth loss “may also reflect life-long socioeconomic disadvantages, such as limited access to and quality of medical and dental care, fewer years of education, and poor nutrition.” Reverse causality is explicitly live — cognitive decline degrades toothbrushing. This is an association, not a cause.
If any of this changed how you think about your own body, an assessment is where that conversation starts.